Medical History:
A 39-year-old male patient presented with complaint of gradually progressive loss of night vision.
Diabetes mellitus (-)
Systemic hypertension (-)
Family history (-)
Smoking (-)
Trauma (-)
Examination Findings
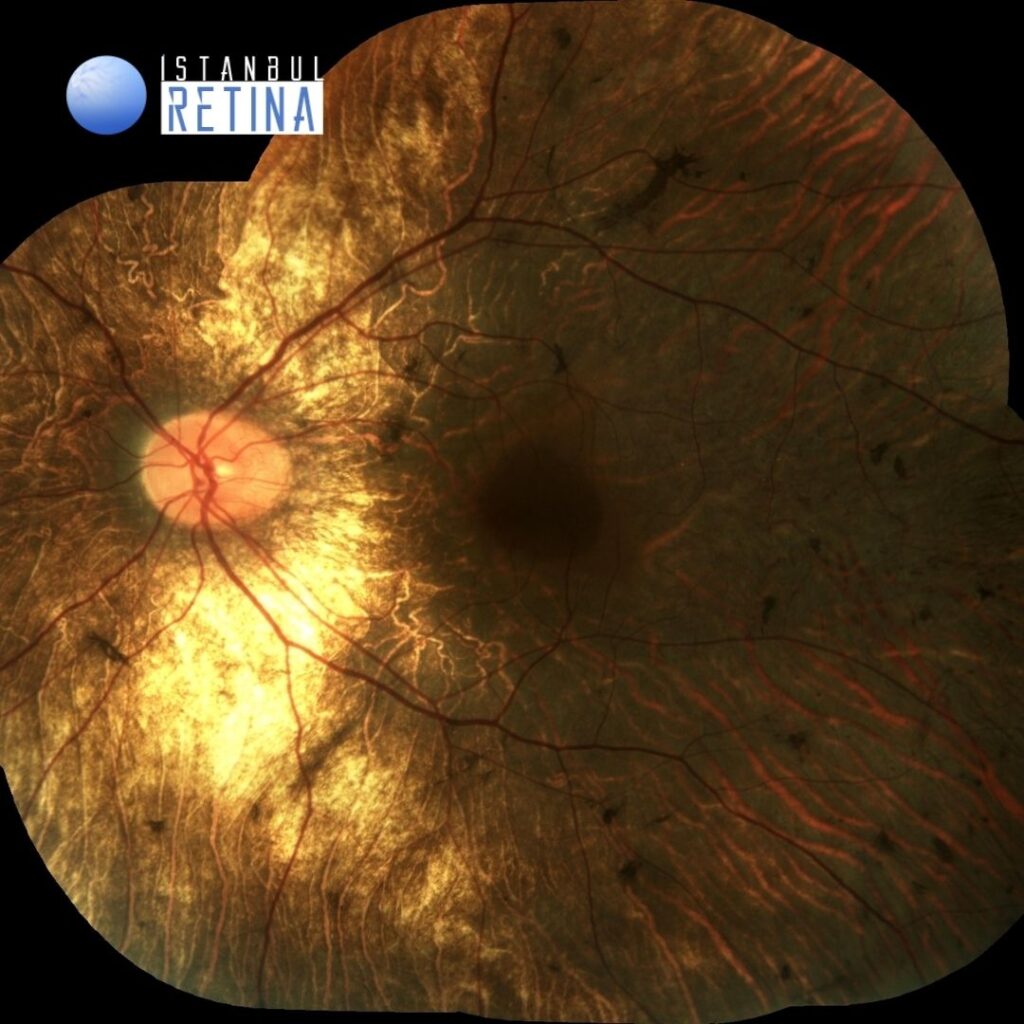
Best corrected visual acuity was 9/10 in the right eye and 9/10 in the left eye. Intraocular pressure was 15 mmHg in both eyes. Anterior segment examination was unremarkable. Funduscopic examination revealed bilateral normal appearing optic nerve head and retinal vessels, widespread pigment clumping, well-defined regions of atrophy with visible underlying sclera and large choroidal vessels, and preserved island of tissue in the fovea (Figure 1).

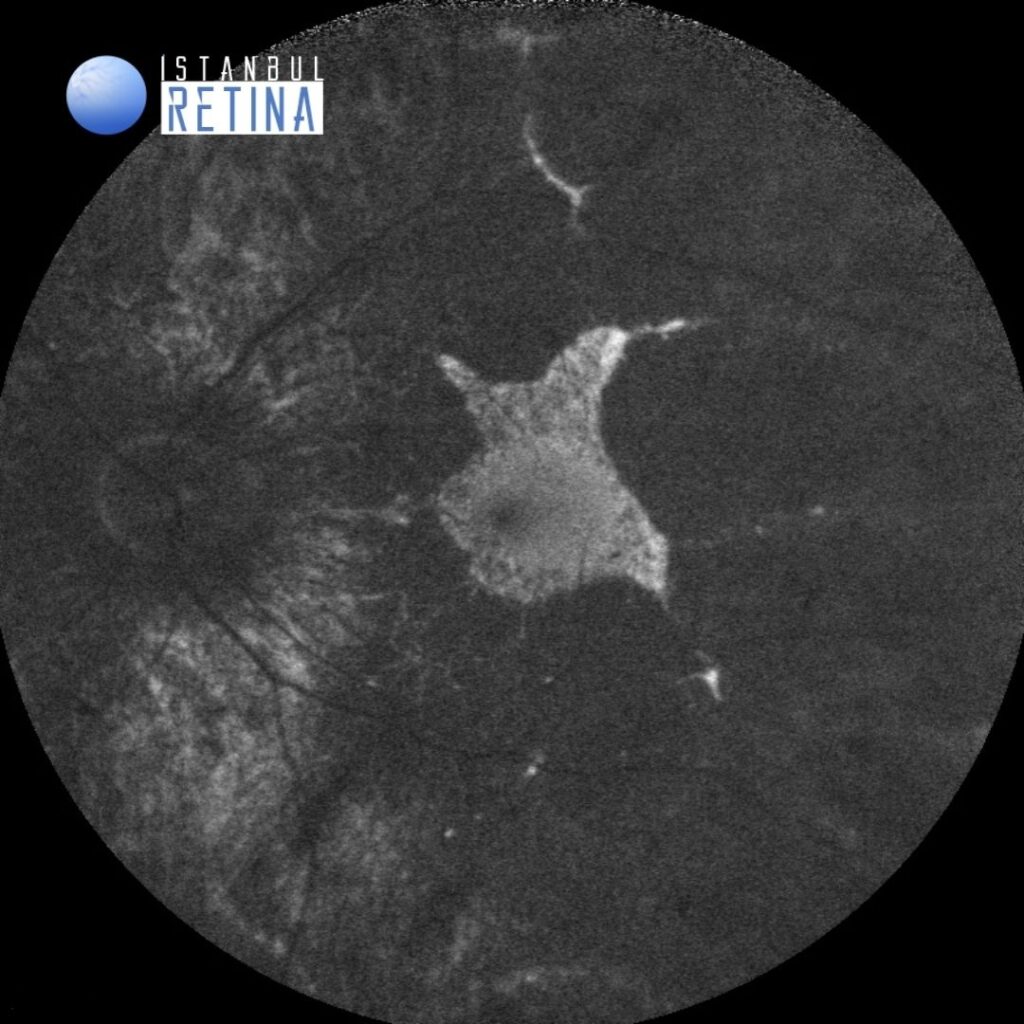
Fundus autofluorescence imaging showed a well-preserved retinal island in the fovea (Figure 2).

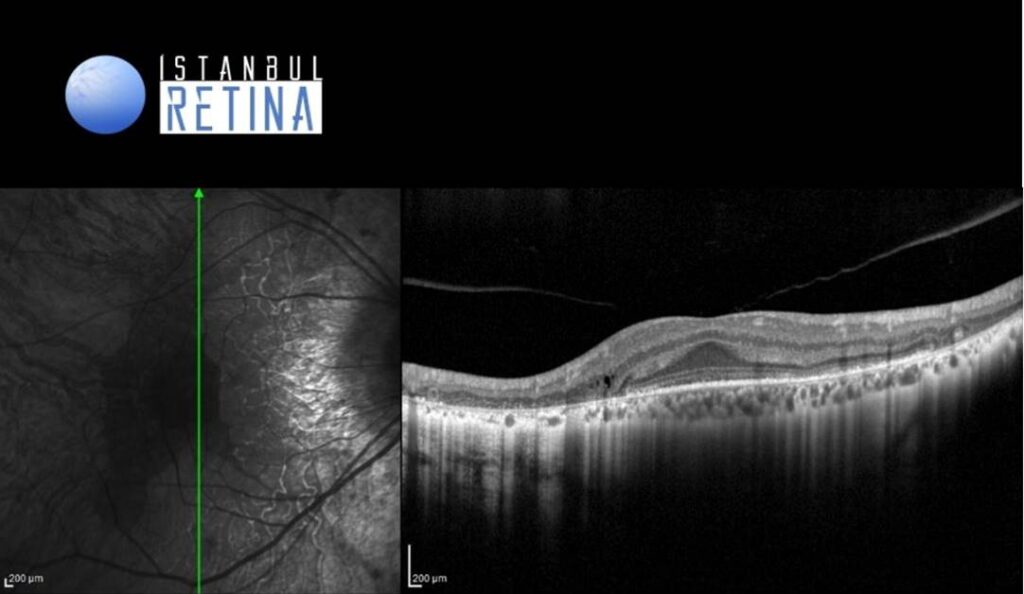
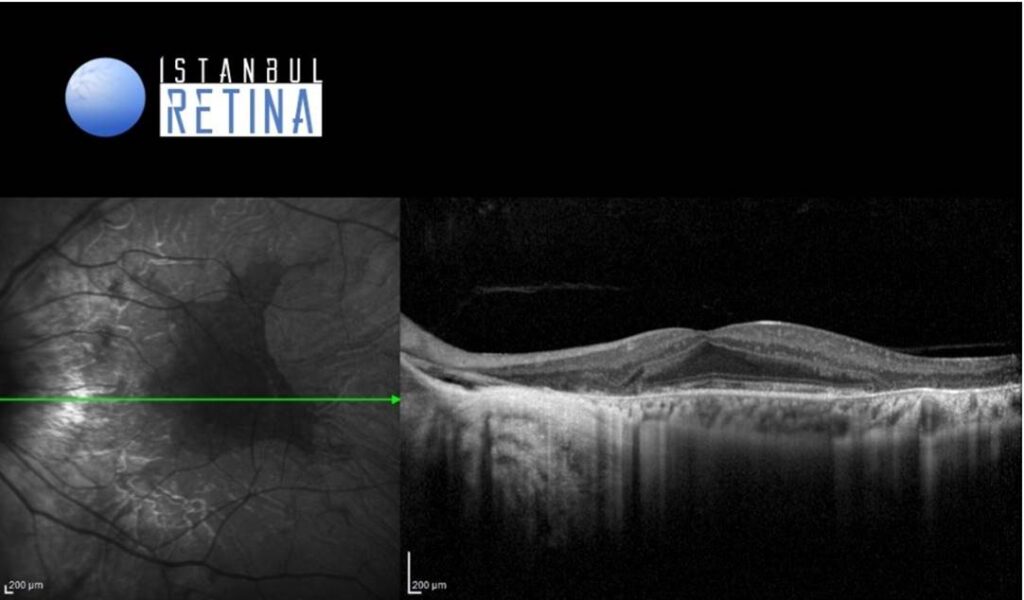
SD-OCT revealed bilateral loss of the external limiting membrane and ellipsoid zone outside the fovea region (Figure 3).
Diagnosis
Choroideremia
Choroideremia is an X-linked chorioretinal dystrophy characterized by the diffuse, progressive degeneration of the retinal pigment epithelium (RPE), photoreceptors and choriocapillaris. Choroideremia is due to various mutations involving the CHM gene and is inherited in an X-linked recessive manner. Men are predominantly affected, but women can be asymptomatic carriers or rarely can be affected by the dystrophy as well.
Choroideremia becomes symptomatic during the first decade of childhood with the development of nyctalopia. It then progresses to peripheral vision loss in teenage years with sparing of central vision and maintenance of good visual acuity until the fifth to seventh decade of life.At around the fifth decade of life, most patients develop a rapid deterioration in central vision.
On fundus examination, the earliest manifestation is widespread pigment clumping, which is distinct from the characteristic perivascular bone-spicule pigment clumping seen in retinitis pigmentosa.Subsequently, patients develop well-defined regions of atrophy with visible underlying sclera and large choroidal vessels, most commonly in the postequatorial region just outside the vascular arcades. These areas of atrophy advance centripetally and are also found in a peripapillary and parapapillary manner. An island of foveal tissue may persist until later stages of the disease when central vision become affected from foveal atrophy. Patients have preserved larger choroidal blood vessels and normal appearing retinal vessels. In addition, choroideremia exhibits no optic atrophy, unlike the waxy pallor of optic discs seen in retinitis pigmentosa.
Differential Diagnosis
Retinitis Pigmentosa, Gyrate atrophy, Bietti crystalline dystrophy
Treatment
There are no currently approved treatments for choroideremia.
References:
1.American Academy of Ophthalmology. Choroideremia https://eyewiki.aao.org/Choroideremia
2.Khan KN, Islam F, Moore AT, Michaelides M. Clinical and Genetic Features of Choroideremia in Childhood. Ophthalmology. 2016:2158-2165. https://pubmed.ncbi.nlm.nih.gov/27506488/
{kind=link}