Medical History:
A 27-year-old male patient with low vision in both eyes was examined in our clinic.
Diabetes mellitus (-)
Systemic hypertension (-)
Family history (-)
Smoking (-)
Trauma (-)
Examination Findings
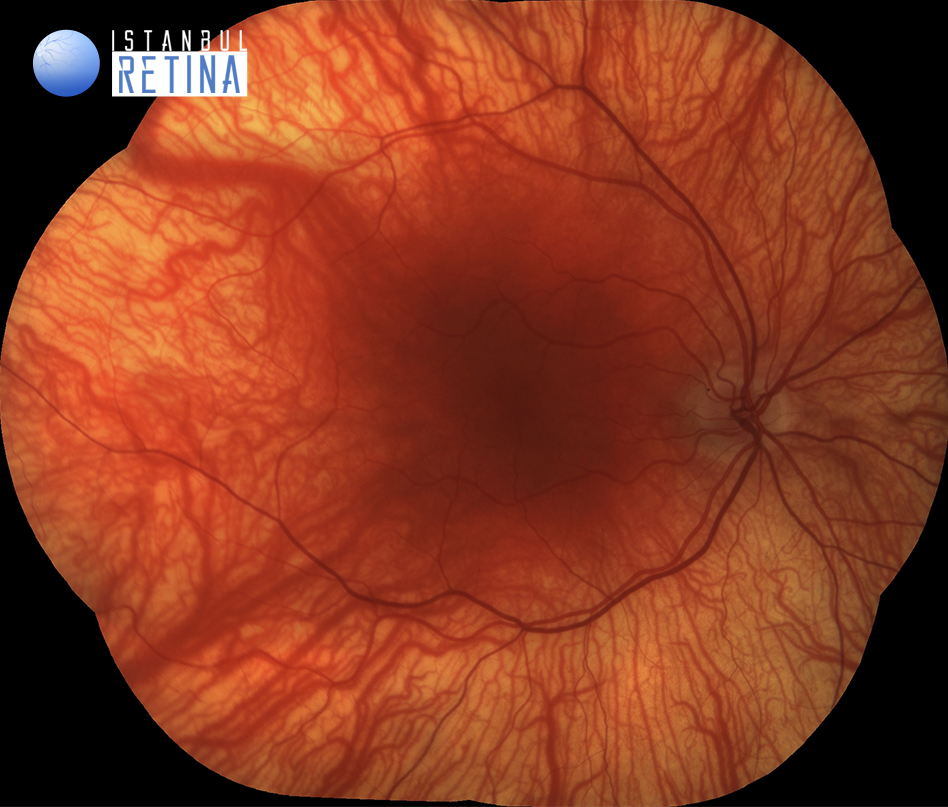
The best corrected visual acuity was 2/10 in both eyes. Intraocular pressure was 15 mmHg in both eyes. Anterior segment examination revealed bilateral iris hypopigmentation. Fundus examination revealed bilateral hypopigmented fundus with prominent choroidal vessels (Figure 1).

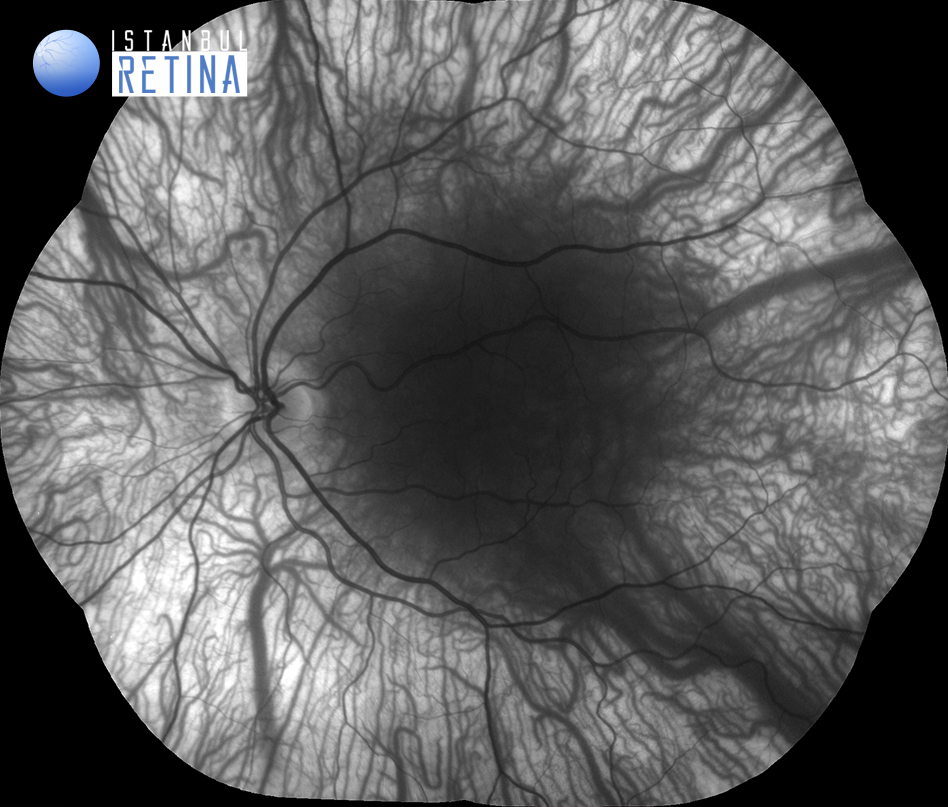
Infrared reflectance imaging shows bilateral prominent choroidal vessels (Figure 2).

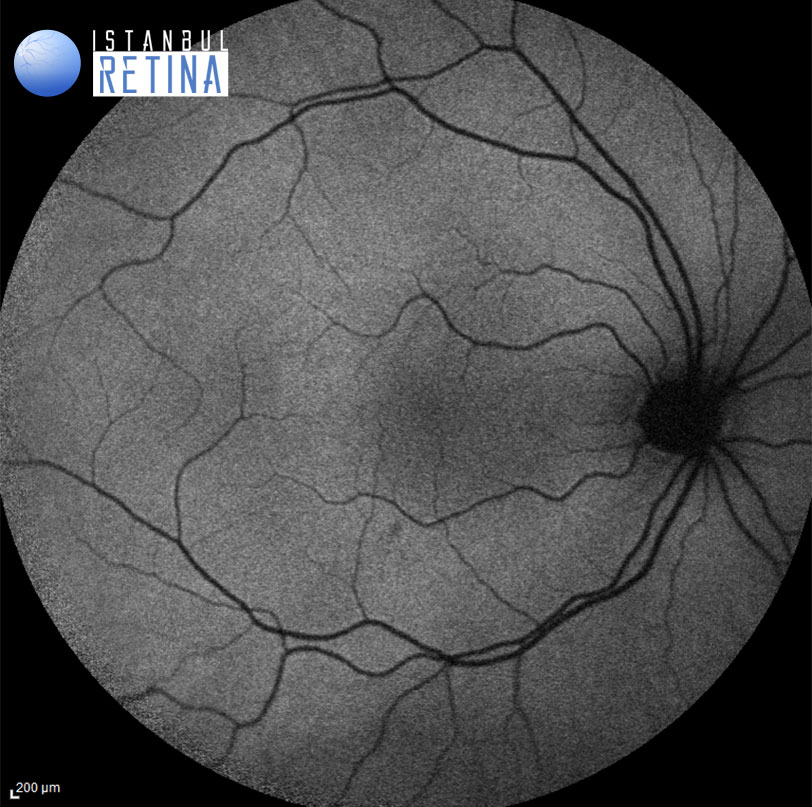
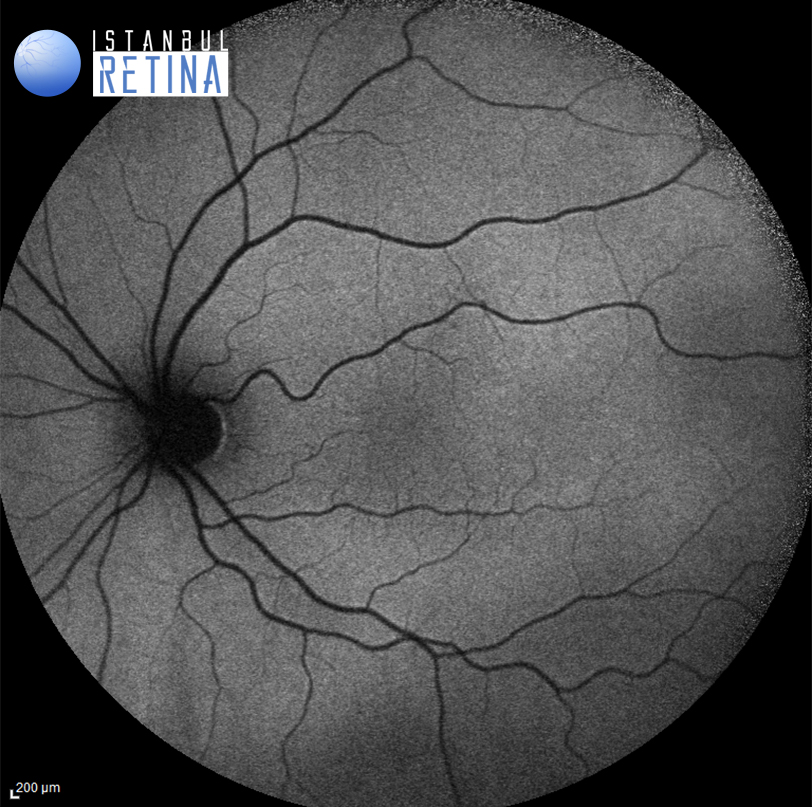
Fundus autofluorescence (FAF) imaging shows bilateral absence of the normal FAF (Figure 3).
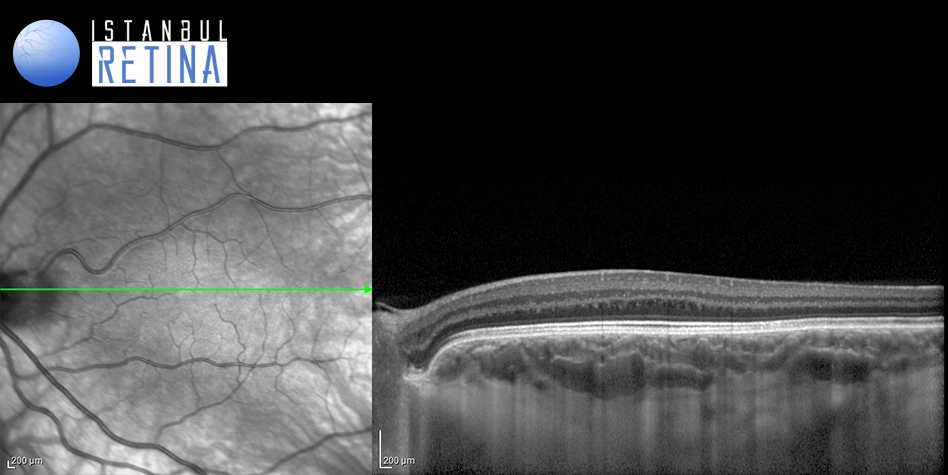
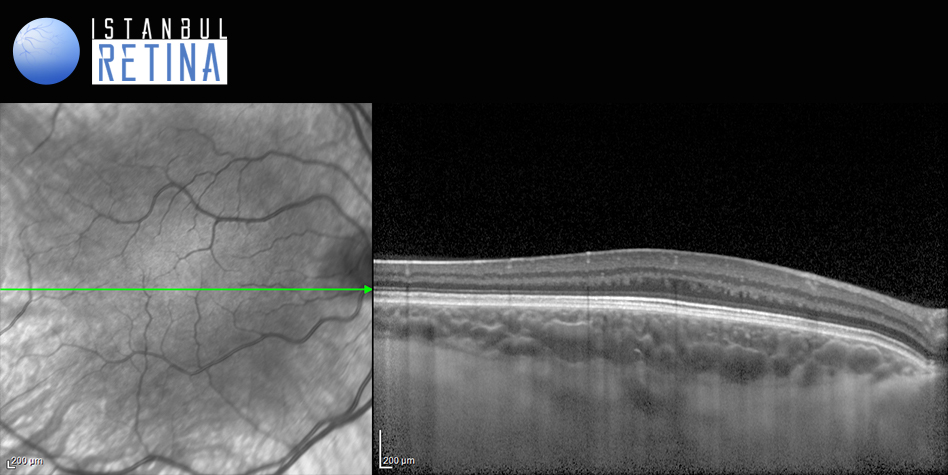
SD-OCT imaging shows bilateral grade 3 foveal hypoplasia (Figure 4).
Diagnosis
Ocular Albinism
Albinism is an inherited disease characterized by a decrease or absence of melanin pigment production. The incidence is between 1: 1000 and 1:20 000. In ocular albinism (X-linked inheritance), only the eyes are involved, while in oculocutaneous albinism (autosomal recessive inheritance), the eyes, hair and skin are affected. Many genetic mutations have been shown to affect the tyrosinase enzyme, which plays a critical role in melanin synthesis. Skin and eye pigmentation does not develop in patients with type I oculocutaneous albinism (tyrosinase negative). In cases of type II oculocutaneous albinism (tyrosinase positive), some pigmentation may occur in the skin and eyes over time.
Structural Grading of Foveal Hypoplasia Using Optical Coherence Tomography:
Grade 1: Shallow foveal pit, presence of outer nuclear layer widening, presence of outer segment lengthening
Grade 2: Grade 1 but absence of foveal pit
Grade 3: Grade 2 but absence of outer segment lengthening
Grade 4: Grade 3 but absence of outer nuclear layer widening
Differential Diagnosis
Differential diagnosis includes oculocutaneous albinism, Hermansky-Pudlak syndrome, Chediak-Higashi syndrome, Griscelli syndrome, and Waardenburg syndrome type II.
Treatment
Currently, there is no genetic or targeted therapies to correct the underlying genetic mutation in ocular albinism.
References
Gargiulo A, Testa F, Rossi S, et al. Molecular and clinical characterization of albinism in a large cohort of Italian patients. Investig Opthalmology Vis Sci 2011;52:1281-1289.https://pubmed.ncbi.nlm.nih.gov/20861488/
Kruijt CC, de Wit GC, Bergen AA, Florijn RJ, Schalij-Delfos NE, van Genderen MM. The Phenotypic Spectrum of Albinism. Ophthalmology 2018;125:1953‐1960.https://pubmed.ncbi.nlm.nih.gov/30098354/
Dorey SE, Neveu MM, Burton LC, Sloper JJ, Holder GE. The clinical features of albinism and their correlation with visual evoked potentials. Br J Ophthalmol 2003;87:767‐772.https://pubmed.ncbi.nlm.nih.gov/12770978/
Creel D, Yu M, Iannaccone A. Characteristics of Visual Electrophysiology in Albinism. In: Yu M., Creel D., Iannaccone A. (eds) Handbook of Clinical Electrophysiology of Vision. 2019. Springer, Cham.
Thomas MG, Kumar A, Mohammad S, et al. Structural grading of foveal hypoplasia using spectral-domain optical coherence tomography a predictor of visual acuity? Ophthalmology 2011;118:1653-1660.https://pubmed.ncbi.nlm.nih.gov/21529956/
{kind=link}