Medical History:
An 26-year-old male patient with a history of Best vitelliform macular dystrophy presents for an examination complaining of decreased vision.
Diabetes mellitus (-)
Systemic hypertension (-)
Family history (+)
Smoking (-)
Trauma (-)
Examination Findings
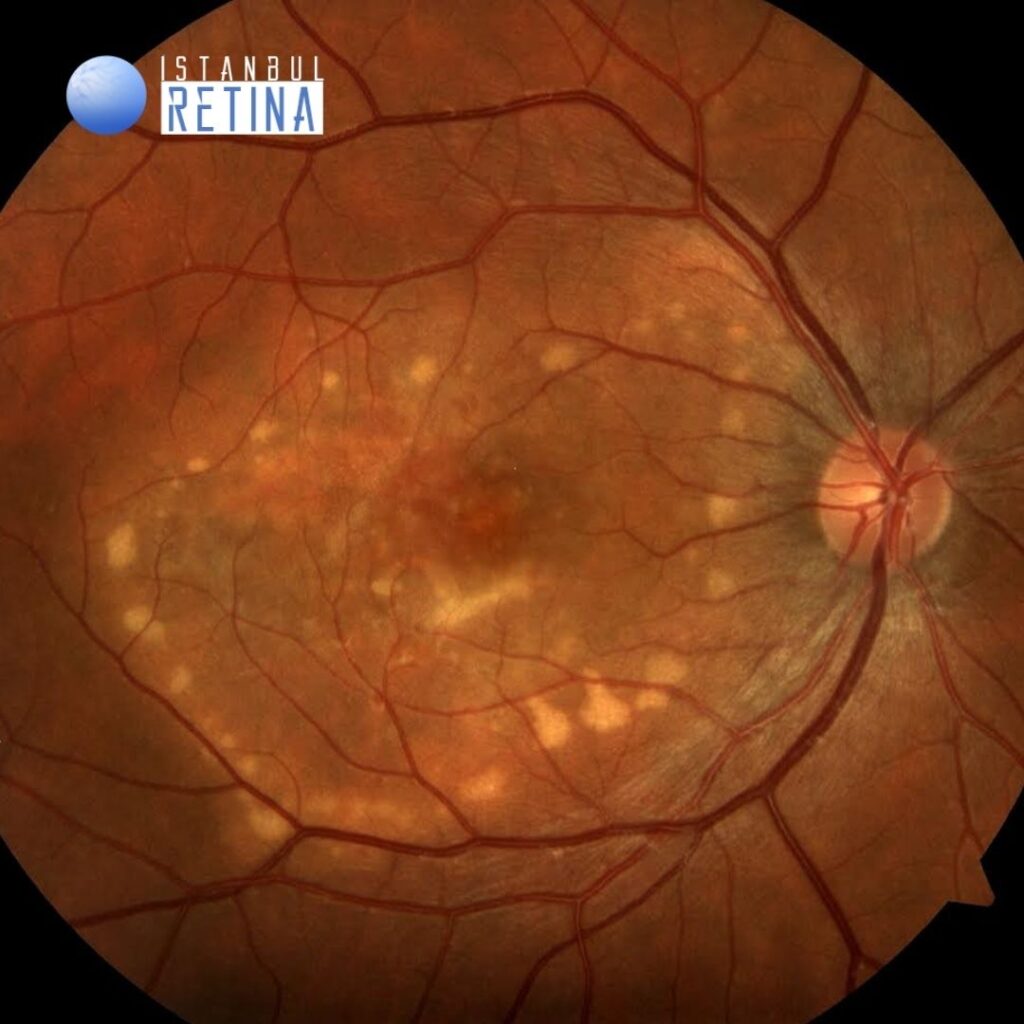
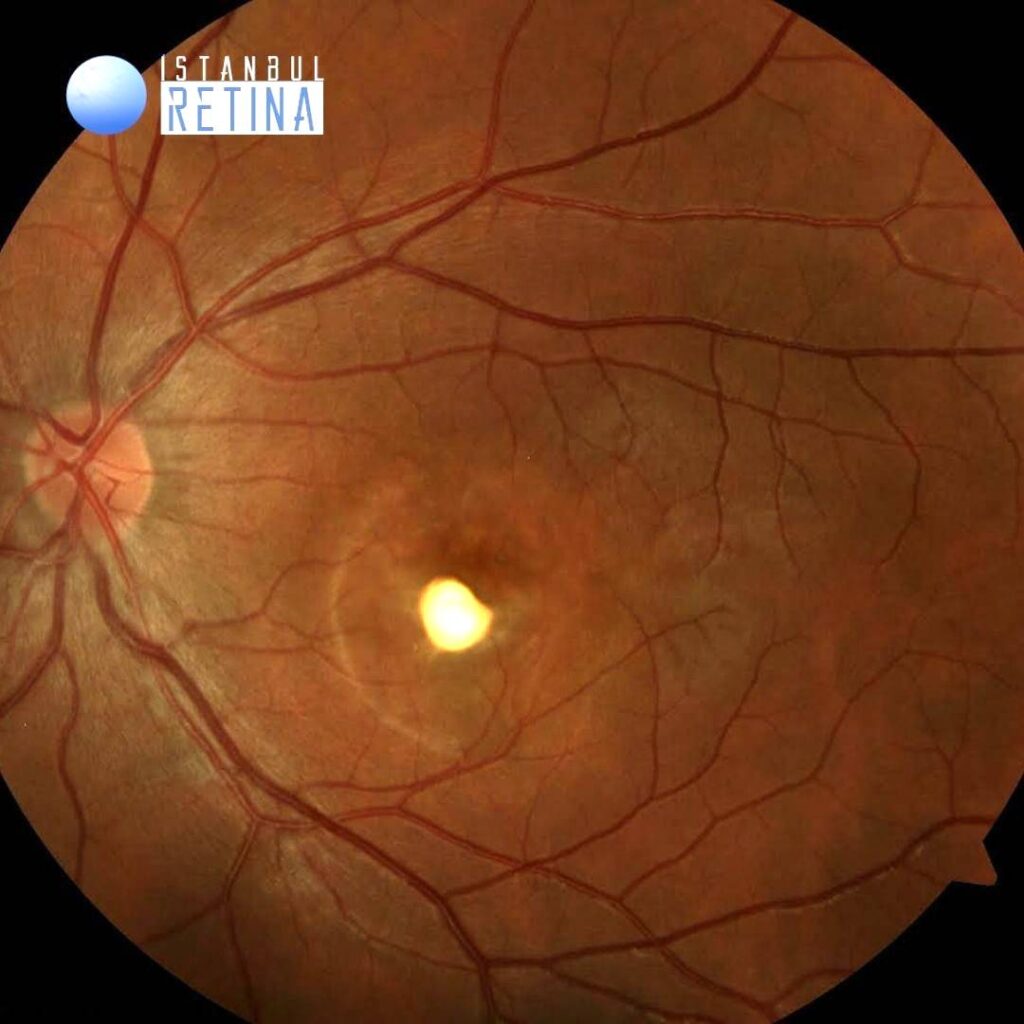
Best corrected visual acuity was 8/10 in the right eye and 2/10 in the left eye. Intraocular pressure was 17 mmHg in both eyes. Anterior segment examination was normal in both eyes. Funduscopic examination revealed bilateral central macular elevation and vitelliform material accumulation, and subretinal fibrosis inferior to the fovea in the left eye (Figure 1).
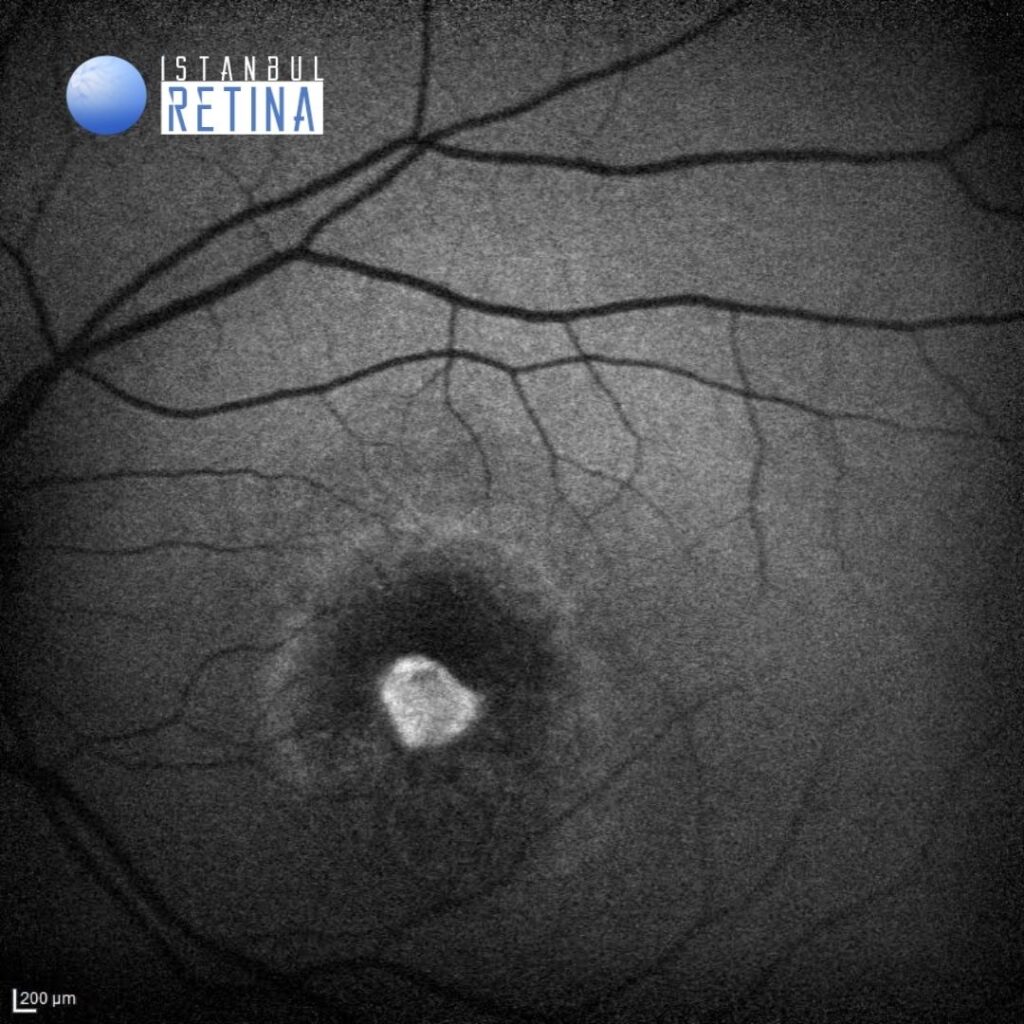
Fundus autofluorescence showed central hypoautofluorescence and hyperautofluorescent ring at the posterior pole in the right eye and central hyperautoflorescent area and hyperautofluorescent ring at the posterior pole in the left eye (Figure 2).

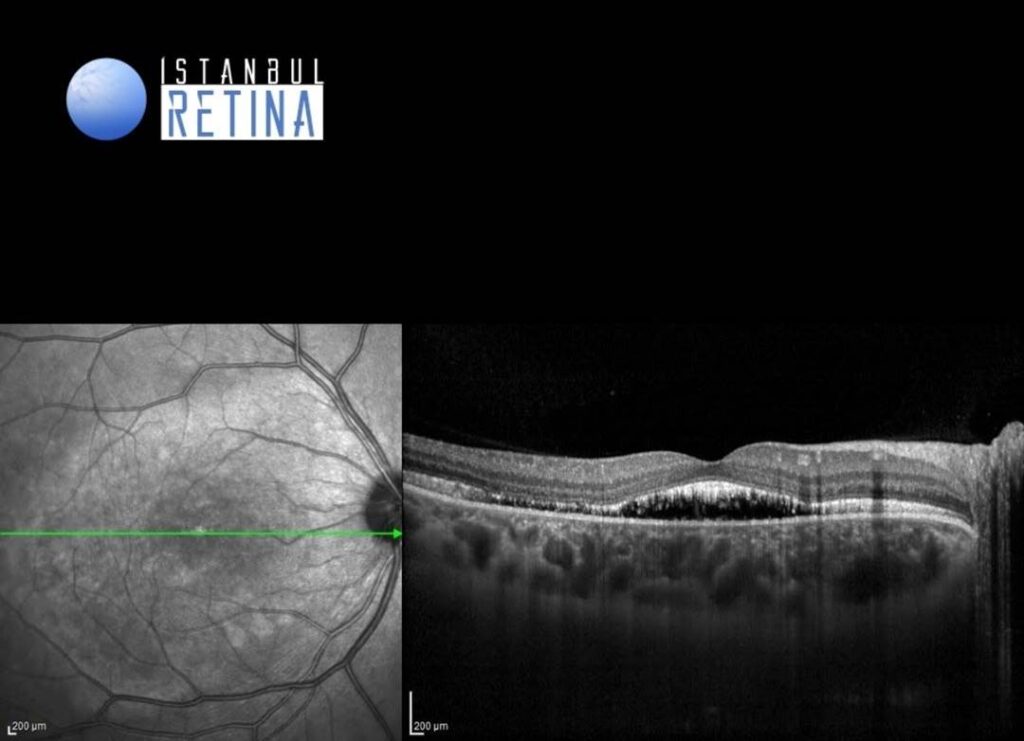
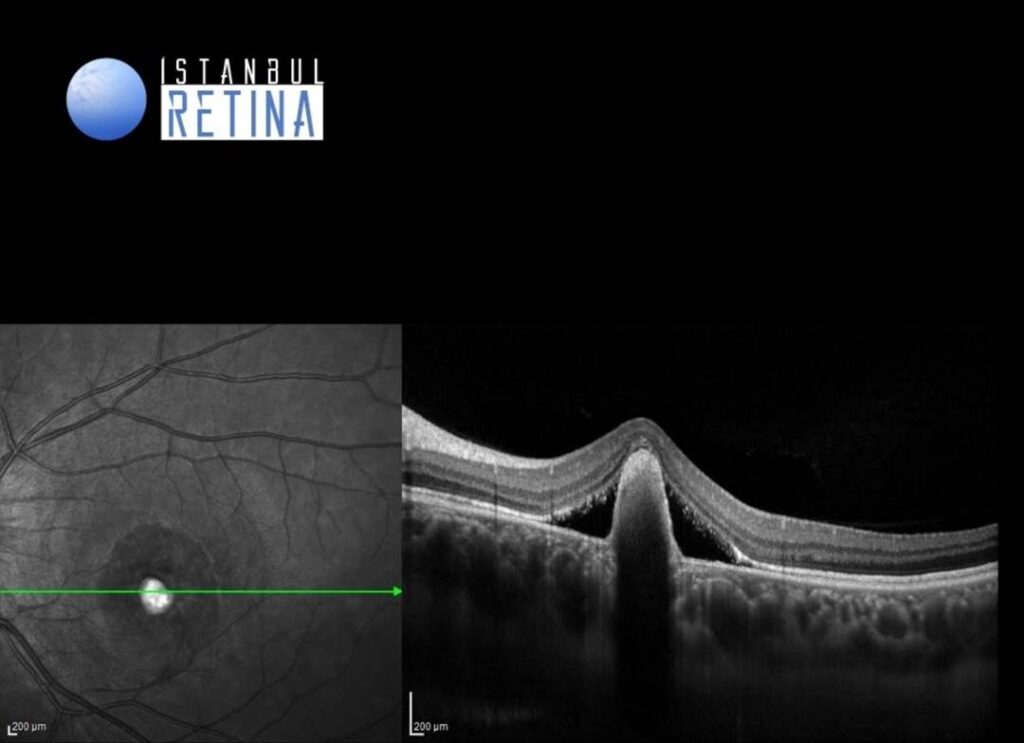
SD-OCT revealed bilateral macular detachment and regular hyperreflective elevation of retinal pigment epithelium inferior-nasal to the fovea in the left eye (Figure 3).
Diagnosis
Best Disease Presenting as Subretinal Pigment Epithelium Hyperreflectivite Lesion on Optical Coherence Tomography
Vitelliform macular dystrophy, also called Best disease, is an inherited retinal dystrophy caused by mutation in the BEST1 gene located on chromosome 11q12–q13. Best disease has a number of distinct stages such as stage I-previtelliform, stage II-vitelliform, stage III-pseudohypopyon, stage IV-vitelliruptive, stage V-atrophic, and stage VI- choroidal neovascularization. But the disease does not progress through each of these stages in every individual. Indeed, the vitelliform stage, in which the macula has a characteristic yellowish appearance due to lipofuscin accumulation at the level of the retinal pigment epithelium (RPE), is frequently not present at the time of examination and sometimes it never occurs.
During the vitelliform stage, diagnosis of Best disease is simple. However, during late stages, confirming the diagnosis by multimodal imaging techniques such as optical coherence tomography (OCT) and fundus autofluorescence is very useful. Although the appearance of lipofuscin accumulation between the RPE and the outer retina is characteristic of Best Disease, presence of hyperreflective material between the RPE and Bruch’s membrane, with serous macular detachment, may be the first presenting finding in some patients. The diagnosis may be controversial in such cases.
Differential Diagnosis
Adult foveomacular vitelliform dystrophy, age related macular degeneration, central serous retinopathy
Treatment
There is no medical or surgical management for Best disease. CNV, however, can be a potentially devastating complication. Application of anti-VEGF therapy for CNV in the setting of Best disease has shown potential for improving outcomes.
References:
Sayman Muslubas I, Arf S, Hocaoglu M, Giray Ersoz M, Karacorlu M. Best disease presenting as subretinal pigment epithelium hyperreflectivite lesion on spectral-domain optical coherence tomography: Multimodal imaging features. Eur J Ophthalmol. 2022;32:2702- 2711. https://pubmed.ncbi.nlm.nih.gov/34806463/
{kind=link}